Mechanically induced switches in the resolution of inflammation
Lead supervisor: S. Uhlig, Co-supervisor: R. Merkel, Junior supervisor: K. Reiss Uniklinik RWTH Aachen, Institute of Pharmacology and Toxicology
Hypothesis: Non-physiological cyclic mechanical stress promotes acute respiratory distress syndrome (ARDS) in the lung by preventing the resolution of inflammation.
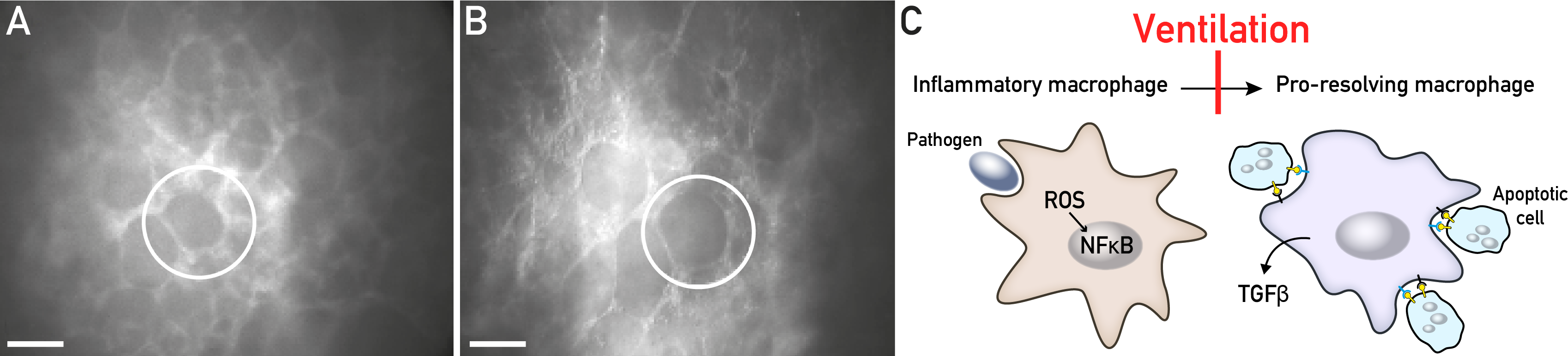
Key aspects of C2. (A, B) Images of ventilated lung slices before and after biaxial stretchingfrom 80. (C) Scheme depicting the inhibition of macrophage conversion by ventilation.
Background: Acute respiratory distress syndrome (ARDS) is a complication frequently observed in intensive care patients with a mortality rate of about 40%. The disease often develops from an acute inflammatory reaction in the first few days to a chronic fibro-proliferative phase. All ARDS patients receive mechanical ventilation, which is life-saving. At the same time, ventilation often causes inflammatory side effects that may increase mortality as suggested in the famous ARDSNet study, which correlated ARDS mortality with inflammation parameters but not with barotrauma, hypoxia or hypercapnia81. This gave great momentum to the biotrauma hypothesis (co-developed by our group82), according to which pulmonary inflammation is promoted by the forces associated with mechanical ventilation. However, after more than 15 years the connection between ventilation, inflammation, fibrosis and mortality in ARDS remains unclear. While it is undisputed that mechanical ventilation may cause inflammation, it has become evident that this alone is not sufficient to cause ARDS-like lung failure83. Thus, the inflammation that is induced by mechanical ventilation must act in a more subtle way. We also need to explain why unventilated experimental animals that survive the acute ARDS phase - unlike many (ventilated) patients - usually recover completely, a process that is dependent on the anti-inflammatory reprogramming of cells, including macrophages and most likely type I and/or type II epithelial cells in the alveolus. We therefore propose that mechanical ventilation sets a mild but persistent pro-inflammatory stimulus that might influence the macrophage-epithelium interaction and prevents the reprogramming of pro-inflammatory M1 into anti-inflammatory M2 macrophages. Aims: We explore the hypothesis that cyclic mechanical signals (such as in mechanical ventilation) provide inflammatory cues that prevent the conversion of pro-inflammatory M1 into anti-inflammatory M2 macrophages directly or by signals derived from epithelial cells. Approach: Epithelial cells and macrophages are stretched (i) in a cell stretcher developed at FZJ61 in order to examine cell-specific effects, (ii) in precision-cut lung slices that are kept in a bioreactor developed in house80 to investigate macrophage polarization and epithelium interaction in intact tissue, and (iii) in an established mouse intensive care unit, where we study the resolution of acute inflammation in mechanically ventilated mice in vivo83. Macrophage origin (blood, alvelous, interstitium) and phenotypes (M1/M2) are characterized by flow cytometric analyses of surface antigens as well as gene and protein expression levels. In addition, we study cell-matrix interactions (podosomes) of macrophages, which are suspected of playing a role in mechanosensing84, and their influence on macrophage polarization.